By Amrita — The Product Scientist
It was 2 AM when I realized we had a problem.
We’d spent three months building a fertility intelligence engine — a system designed to synthesize clinical biomarkers, Ayurvedic phenotyping signals, and lifestyle data into actionable reproductive health recommendations. The prototype was promising. The LLM underneath was brilliant at reasoning. But when a test query asked about the interaction between AMH levels and thyroid antibodies in unexplained infertility, it hallucinated a clinical guideline that didn’t exist.
That hallucination could have reached a real couple. A couple already navigating the emotional weight of infertility. A couple who would have trusted us because we positioned ourselves as the intelligent layer between them and clinical complexity.
That night forced a question every medical AI builder eventually faces: do we teach the model to know medicine, or do we teach it to look things up?
That’s the fine-tuning vs. RAG decision. And if you’re building in healthcare, getting it wrong isn’t a product issue — it’s a patient safety issue.
What fine-tuning actually does
Fine-tuning is, at its core, a form of medical education for a machine.
Think of a base large language model as a brilliant medical graduate — someone who has read everything, understands language and reasoning at an extraordinary level, but has never done a clinical rotation. They know about medicine the way someone knows about a country they’ve never visited: broad familiarity, zero operational depth.
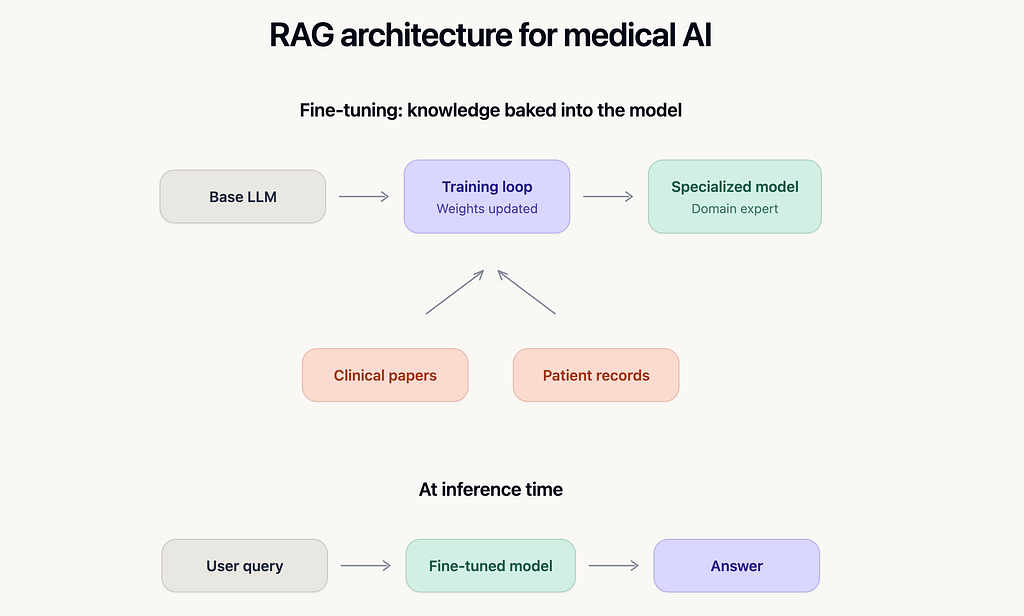
Fine-tuning is the residency. You take this general-purpose model and run it through thousands — sometimes hundreds of thousands — of domain-specific training examples. Clinical trial reports, annotated patient records, diagnostic decision trees, pharmacological interaction databases. The model’s internal parameters (its “weights”) shift. The neural pathways that fire when it encounters medical language become sharper, more specialized.
After fine-tuning, the model doesn’t look up the answer. It knows the answer, the way a senior clinician knows it — encoded in its parameters, accessible instantly, shaped by the patterns in its training data.
The architecture is deceptively simple: base model in, domain-specific training data applied, specialized model out. At inference time, there’s no retrieval step, no external database call. The user asks a question, and the fine-tuned model generates a response from its internalized knowledge.
A concrete example: clinical language normalization
Consider a fertility health system that needs to interpret lab reports from dozens of pathology labs across India and the Middle East. The same biomarker — Anti-Müllerian Hormone — appears as “AMH,” “Anti Mullerian Hormone,” “Hormone anti-mullérienne,” “serum AMH (ECLIA),” and half a dozen other variants, often with different reference ranges and unit conventions.
A base LLM handles some of this, but inconsistently. It might map “AMH” correctly but stumble on “Hormone anti-mullérienne” because its general training data underrepresents French-language pathology reports.
A fine-tuned model trained on 50,000 annotated lab reports learns to normalize all of these into a canonical representation. It doesn’t need to retrieve a mapping table — the mapping lives inside the model. The response is faster, the latency is lower, and the behavior is consistent because the knowledge is baked into the weights.
This is where fine-tuning shines: when the knowledge is stable, the vocabulary is specialized, and you need the model to speak the domain’s language natively rather than translating on the fly.
The cost you pay
Fine-tuning isn’t free, and the costs aren’t just computational.
First, you need high-quality labeled data — and in healthcare, that data is expensive, sensitive, and regulated. Annotating clinical records requires domain experts. De-identification must be bulletproof. IRB and ethics review cycles can stretch for months.
Second, knowledge freezes at training time. If NICE updates its fertility treatment guidelines tomorrow, your fine-tuned model doesn’t know about it until you retrain. In a domain where a single updated meta-analysis can change clinical practice, this staleness is a genuine risk.
Third, fine-tuned models can hallucinate with more confidence. A base model hedges when it’s unsure. A fine-tuned model has learned the style of clinical authority — so when it fabricates an answer, it does so in the voice of a confident clinician. This is arguably more dangerous than a generic hallucination because downstream users are less likely to question it.
What RAG actually does
Retrieval-Augmented Generation takes the opposite philosophical stance. Instead of teaching the model to memorize, you teach it to research.
The mental model I find most useful: RAG turns an LLM into a clinician with a perfectly organized reference library and the discipline to consult it before answering every single question.
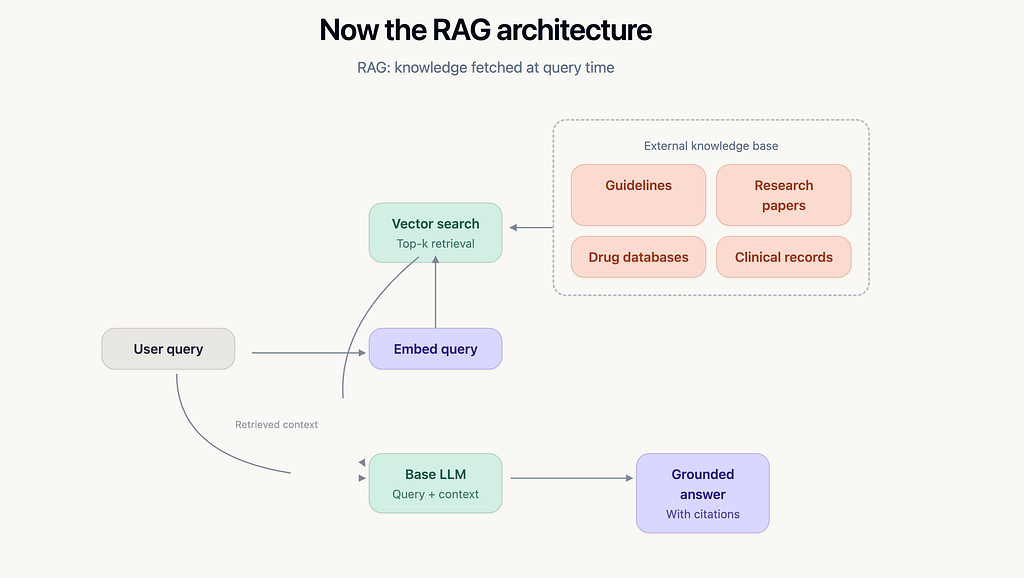
Here’s what happens mechanically. When a user submits a query, the system first converts that query into a vector embedding — a numerical representation of its semantic meaning. This embedding is compared against a pre-indexed knowledge base (clinical guidelines, research papers, drug interaction databases, your own curated content) using vector similarity search. The top-k most relevant chunks of text are retrieved and injected into the LLM’s prompt alongside the user’s original question. The model then generates a response grounded in those retrieved documents.
The critical insight: the LLM itself is unchanged. You’re using a general-purpose model, but you’re controlling what information it has access to at the moment of generation. The knowledge lives in the external database, not in the model’s weights.
A concrete example: treatment protocol recommendations
A couple comes to your platform with a specific clinical profile: female partner, age 34, AMH 1.2 ng/mL, BMI 27, history of one failed IUI cycle. Male partner, normal semen analysis but borderline morphology at 3%.
The question: what does the evidence say about their next step — another IUI with ovarian stimulation, or direct escalation to IVF?
This is exactly the kind of question where RAG excels. The answer depends on the latest clinical evidence — ESHRE guidelines updated in 2024, the most recent Cochrane review on IUI vs. IVF for unexplained subfertility, and possibly emerging data on the predictive value of AMH thresholds in treatment selection.
A RAG system retrieves the relevant guideline sections, the key findings from the Cochrane review, and any indexed studies matching this clinical profile. It passes these to the LLM with instructions to synthesize a recommendation grounded in the retrieved evidence. The output isn’t the model’s opinion — it’s a synthesis of the sources, and every claim can be traced back to a specific document.
If ESHRE updates their guidelines next month, you update the knowledge base. No retraining. No GPU hours. The next query automatically retrieves the new guidance.
The cost you pay
RAG has its own failure modes, and they’re subtle.
Retrieval quality is the bottleneck. If the vector search returns irrelevant chunks — because the embedding model doesn’t capture clinical nuance well, or because the knowledge base is poorly chunked — the LLM will generate a confident answer grounded in the wrong evidence. Garbage in, eloquent garbage out.
Latency increases. Every query now involves an embedding step, a vector search, and a longer prompt. For real-time clinical decision support, this latency matters.
Context window limits impose hard constraints. You can only inject so many retrieved chunks before you hit the model’s context window ceiling. For complex clinical questions that require synthesizing across multiple guidelines, multiple studies, and patient-specific history, you may not be able to fit everything the model needs to see.
And the integration engineering is non-trivial. Building a reliable RAG pipeline for healthcare means solving chunking strategy (how do you split a 200-page clinical guideline into retrievable units without losing context?), embedding model selection (general-purpose embeddings vs. biomedical embeddings like PubMedBERT), re-ranking (the top-k by cosine similarity aren’t always the top-k by clinical relevance), and guardrails (what happens when retrieval returns nothing relevant — does the model admit it, or confabulate?).
The decision framework I actually use
After building across both paradigms, here’s the honest heuristic:
Fine-tune when the knowledge is stable and the task is specialized. Clinical language normalization, medical entity extraction, phenotype classification, triage logic — these are tasks where the vocabulary and decision boundaries don’t shift monthly. The model needs to internalize a way of thinking, not access a reference library.
Use RAG when the knowledge is dynamic and traceability matters. Treatment recommendations, drug interaction checks, guideline-based decision support, evidence synthesis — these are domains where the source matters as much as the answer. Clinicians (and regulators) need to see where the recommendation came from. And the evidence base updates faster than any retraining cycle.
In practice, production medical AI systems use both.
At Ovviia (os.ovviia.com), our approach reflects this. The clinical language layer — the system that normalizes biomarker representations, maps Ayurvedic phenotyping signals to clinical correlates, and classifies couple-level fertility profiles — benefits from fine-tuning. This is stable, specialized knowledge that the model needs to handle natively and at speed.
But the recommendation engine — the layer that synthesizes evidence-based guidance for a specific couple’s profile — runs on RAG. It pulls from our curated clinical knowledge bank of 1,500+ recommendations, current ESHRE and ASRM guidelines, and indexed research. Every recommendation traces back to a source. When the evidence changes, the knowledge base updates without touching the model.
This isn’t a theoretical architecture. It’s a design decision that emerges from taking patient safety seriously — from recognizing that in reproductive health, a hallucinated recommendation doesn’t just erode trust; it can alter the trajectory of someone’s family-building journey.
The question that matters
The fine-tuning vs. RAG debate is useful, but it’s ultimately a means question. The ends question is harder: does your system know when it doesn’t know?
Neither architecture solves this on its own. A fine-tuned model can hallucinate with clinical authority. A RAG system can retrieve irrelevant evidence and synthesize a plausible-sounding wrong answer. The real engineering challenge — the one that separates medical AI products that earn clinical trust from those that don’t — is building the uncertainty layer on top.
That’s calibration. That’s knowing when to say “I don’t have enough evidence to recommend this.” That’s treating epistemic humility not as a nice-to-have but as a core product requirement.
If you’re building in healthcare AI, the architecture decision is table stakes. The trust decision is what defines your product.
Fine-Tuning vs. RAG for Medical AI: A Builder’s Honest Guide was originally published in Towards AI on Medium, where people are continuing the conversation by highlighting and responding to this story.